This blog post is the last in a series that we are writing in the lead up to the 2018 Behavioural Exchange. It outlines our recent work in health, which is the focus of one of the breakout sessions. As health has been an area that we’ve worked in for a while, we wanted to talk about the work that we’ve done in this area in the UK and in our Sydney office. Our lead in Health, Hugo Harper, joins us to talk about this with Alex Gyani, Principal Advisor at our Sydney Office.
Alex: Over the last eight years, we’ve worked a lot on health – both in the UK and here in Australia. In fact, health was the topic of the first paper BIT ever published, back in 2010. Hugo, how much more do we need to do to integrate behavioural insights into the health systems of the UK and Australia?
Hugo: I’d like to pass the buck back to you for Australia! But the point that you raise about scaling BI-informed health interventions is an important one. Health practitioners have been puzzling over how to take good practices to scale for many years now. There is a well-known saying that it takes 17 years for research evidence to reach clinical practice.
Alex: Do you think this problem is unique to health?
Hugo: No, but the problem with health is that you have some quite complex organisational structures on the one hand, and some engrained professional practices on the other. That’s not to say things can’t be done. In the UK, we recently managed to take a new intervention all the way from initial idea, to pilot, to nationwide scale.
Alex: OK, so what was the intervention?
Hugo: Well, as in many health systems, some hospitals in the UK have pretty long waiting times for non-urgent treatment. And in many cases, patients could wait less if they chose another nearby hospital. But the waiting times are not obvious to doctors or patients at the moment of decision.
Alex: In terms of our EAST framework, it sounds like you could make this information more “Timely” for doctors.
Hugo: That’s right. Working with NHS Digital, we changed the screen that doctors and patients see when making appointments. We inserted a red Limited Capacity alert next to hospitals that had very long waiting times. At the same time, we put all the local providers with good capacity in a big green box at the top of the screen, you can see them in the pictures below. So we made the information easy to understand, at the right time, while still letting people choose long waiting times if they wanted. It’s a classic nudge.
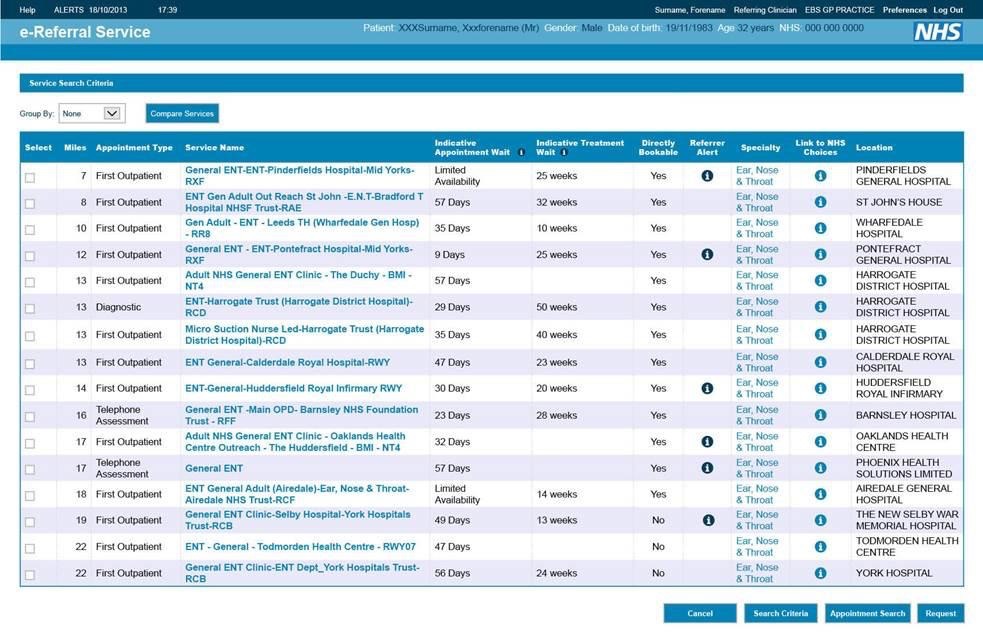
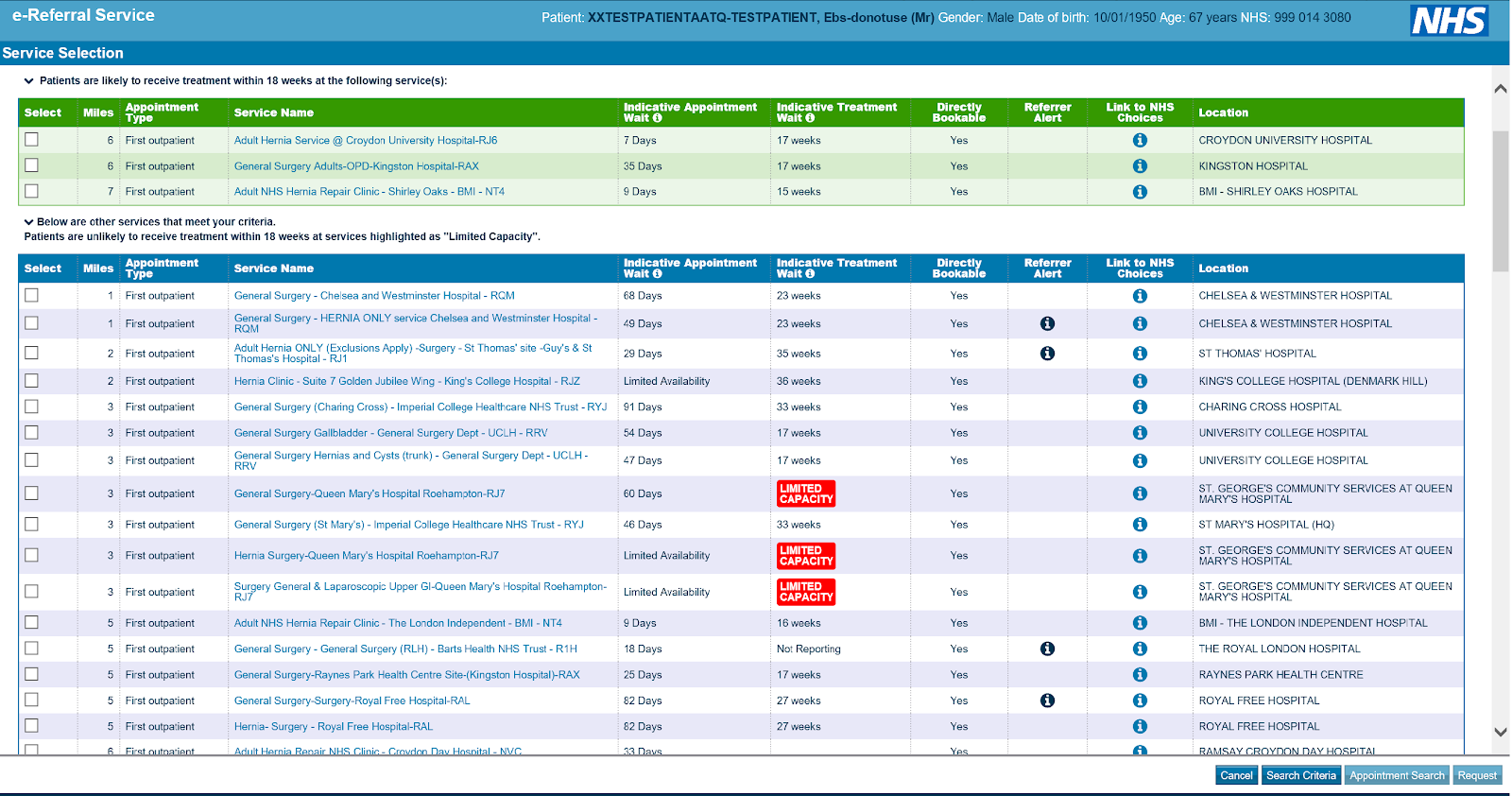 Before and after screenshots of the e-Referrals System, which we adapted in partnership with NHS Digital.
Before and after screenshots of the e-Referrals System, which we adapted in partnership with NHS Digital.
Alex: And what happened?
Hugo: We ran two separate trials to test this change. We found that the proportion of patients choosing hospitals with red alerts fell by around a third. We also found that more people were choosing the hospitals with green alerts. What’s great is that this was built into the nationwide electronic system, so it had a direct route to scaling – which is what’s happening.
Alex: That was a recent project. How are things doing in terms of scaling older solutions?
Hugo: Well, we were lucky enough to run some projects at full scale straight away. For example, our work on reducing antibiotic prescribing was a nationwide intervention that included all general practitioners in England.
But sometimes we have hit a bit of a brick wall. For example, one of our projects from 2014 showed that you could get 25% fewer missed hospital appointments by just changing reminder messages. This is a free intervention with proven results. Quite a few hospitals have taken it up now. But there are still a whole bunch of hospitals who don’t seem to be interested, even though it looks like the costs are low.
Alex: We’ve also trialled a very similar intervention here in Sydney. When we first came over to Sydney to support the development of the Behavioural Insights Unit in the Department of Premier and Cabinet, there was a big question as to whether the same interventions from the UK would scale.
Hugo: And did they?
Alex: Yes! And by testing the concept further we were able to see that the messages that emphasised that by showing up to your appointment the costs can be avoided, were more effective than those that emphasised that not showing up costs the hospital money.
It’s a subtle but important difference. One emphasises what you should do and the other what you shouldn’t do. We also found that there were differences in the way in which certain groups of people responded to the different messages. I wrote about on the Behavioural Insights Unit’s blog here.
Hugo: How did you go about scaling those findings?
Alex: We’ve also had similar results to you when we were trying to get other hospitals to scale the interventions. After we finished the project with the BIU and published the results, some hospitals decided to implement the new messages themselves. From what we gather, they’ve had similar results. However, this model of dissemination relies on hospitals having some driven staff who are willing to be early adopters. If we just rely on dissemination as a method of getting results out there, then we can’t expect everyone to receive the benefits of these interventions. This is partly because people are busy and can’t be expected to read through all the government reports and peer-reviewed journals on effective interventions.
Hugo: Isn’t that exactly why people often don’t follow through on other behaviours like: going to the gym, eating more healthily or saving more money?
Alex: That’s exactly it. There are of course other reasons why effective interventions aren’t being taken up. For example, we also know that local context is important. That is a core tenet of Behavioural Science, but it is as important when considering how your interventions scale, as when you’re designing an intervention. However, that isn’t enough. We often also need more active methods. We’ll be talking through these methods in a little bit more detail in our session on scaling at BX2018, on Monday morning at 11am.